The Emergency Department often presents us with puzzles disguised as common complaints. Some announce themselves loudly through abnormal vitals and dramatic clinical findings. Others remain deceptively quiet, hiding behind normal investigations and reassuring numbers.
This was one such case.
A 34-year-old woman presented to the Emergency Department with severe lower abdominal pain that had begun the previous day and had progressively worsened over the last few hours. The pain was predominantly localized to the lower abdomen, radiating to the back, and was associated with mild giddiness.
Prior to arriving at our Emergency Department, she had sought treatment at another healthcare facility where she received Buscopan and Paracetamol. Despite symptomatic treatment, the pain persisted without significant relief.
She denied fever, vomiting, urinary complaints, vaginal bleeding, vaginal discharge, trauma, or episodes of syncope. Her menstrual cycles were monthly regular and home urine pregnancy card test performed prior to presentation was reported as negative.
On initial assessment, she appeared comfortable and was hemodynamically stable.
Nothing in her vital signs suggested an impending emergency.
However, abdominal examination told a slightly different story.
There was localized tenderness over the left iliac fossa and suprapubic region, without guarding, rigidity, or signs of generalized peritonitis.
Routine laboratory investigations including complete blood count, renal function tests, and electrolytes were within normal limits. The laboratory profile offered little explanation for the intensity and persistence of her symptoms.
Yet something about the clinical picture felt incomplete.
Persistent pain despite analgesics. Localized tenderness. Normal blood work.
The pieces didn’t quite fit.
Given the ongoing symptoms, an urgent ultrasound of the abdomen and pelvis (Transabdominal and Transvaginal) was performed.
The answer finally emerged.
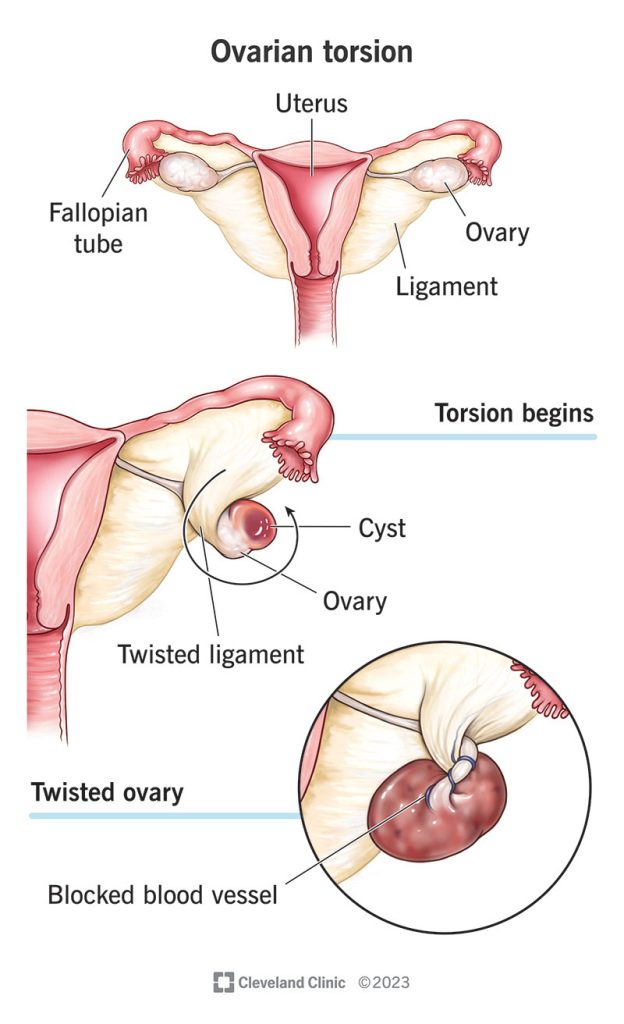
Ultrasound demonstrated a well-defined left adnexal cyst measuring approximately 4 × 7.3 × 5 cm, associated with twisting of the left ovarian pedicle. Although venous flow was still appreciated, the overall sonographic appearance was highly suggestive of left ovarian torsion secondary to a large ovarian cyst.
The mystery had been untwisted.
Immediate gynaecologist opinion was sought and shifted to OT for Laparoscopic salphingoopherectomy.
One of the most important lessons from this case is the misconception that preserved Doppler flow excludes ovarian torsion. In reality, the ovary possesses a dual blood supply, and partial or intermittent torsion may continue to demonstrate detectable flow. Reliance on Doppler findings alone can therefore be misleading.
Ovarian torsion remains a diagnosis that demands careful correlation between clinical suspicion and imaging findings.
Delay in recognition can lead to ovarian ischemia, infarction, necrosis, loss of ovarian function, and potential fertility consequences. Early diagnosis and prompt gynecological intervention remain the cornerstone of successful management.
Take-Home Message
Not every acute abdomen arrives with alarming investigations.
Not every surgical emergency presents with abnormal vital signs.
Sometimes the diagnosis hides behind a normal blood report, a reassuring Doppler signal, and a seemingly uncomplicated ovarian cyst.
For the Emergency Physician, the challenge lies in recognizing when the story doesn’t fit the numbers.
Acute abdominal pain in women of reproductive age remains one of the most challenging presentations in the Emergency Department. While many causes are benign, a subset of conditions demands rapid recognition because delayed intervention can lead to irreversible organ damage. This case serves as a reminder that meticulous clinical assessment, combined with timely imaging, can uncover diagnoses that may otherwise remain hidden.
Time is Ovary.
Authored by
Dr. Sherin Stanly
Emergency Medicine Trainee
Under the Guidance of
Dr. Anjum Akbar Mujawar
Consultant Emergency Medicine
MBBS MEM FEM PEM CCEBDM