The Silent Pandemic | THE TIME BOMB IN YOUR “MIDDLE”
Startling Facts:
- 1 billion people are living with Obesity today
- 1 in 2 people (50%) of the global population will be obese or Overweight by 2035
- 3.23 Lac Crores USD – Estimated impact of overweight and obesity by 2030
- 40 Crore children and adolescents are obese / overweight
- 1.7 Crore premature Non Communicable Disease (NCD) deaths due to overweight / obesity annually
The Greatest Threat to Our Health
On the occasion of World Obesity Day 2026, as a physician with a keen interest in preventive health, clinical nutrition and fitness, I am rarely prone to hyperbole. But today, I am genuinely anxious.
We spent the last few years living in fear of a viral pandemic that swept the globe in months. Yet, we are currently drowning in a much slower, much deadlier “silent pandemic” that is claiming lives at a rate comparable to COVID-19, but without the daily news tickers or the public urgency.
Obesity has moved beyond the affluent West and is now suffocating the developing world. We are seeing it in your clinics / OPDs, our schools, and our morgues. If you think this is just about “carrying a few extra kilos,” you are dangerously mistaken.
The Evolutionary Mismatch: We Weren’t Built for This
Our ancestors survived for millennia because their bodies were masters of storage. Food was scarce, seasonal, and required immense physical effort to obtain. There were no refrigerators to preserve a kill or a harvest; you ate what you had, and then you fasted until the next find.
Today, we live in an environment our DNA doesn’t recognize. We have constant access to high-calorie, low-nutrient food. The “three meals a day” plus snacks model isn’t a biological requirement – it’s a social construct largely fueled by the food industry to keep consumption constant. We have replaced the natural cycle of “feast and famine” with “feast and feast.”
The South East Asian Reality Check: the Rules are Different
We have normalized larger bodies to the point where we can no longer see the medical danger right in front of us. We categorize this risk using the Body Mass Index (BMI), and the escalations are steep. If you are of South East Asian descent, the standard BMI charts you see in Western media are giving you a false sense of security. Your genetic risk for cardiovascular disease and Type 2 Diabetes is significantly higher at lower weights.
Because South East Asians are prone to “thin-outside-fat-inside” (TOFI) phenotypes, you may carry dangerous visceral fat even if you don’t look “large.” Consequently, the BMI cut-offs for Asian populations are much stricter:
- Normal: 18.5 – 22.9: Healthy – Health risk LOW
- Overweight (BMI 23–24.9): The “warning light” on our dashboard – Health risk INCREASED
- Obesity Class I (BMI 25–29.9): The engine is overheating. Chronic inflammation begins to damage every organ system – Health risk HIGH
- Obesity Class II (BMI 30 – 39.9): Health risk VERY HIGH
- Obesity Class III (BMI >40): A state of medical EMERGENCY where life expectancy is drastically shortened
Calculating Our Body Mass Index:
We can calculate our Body Mass Index (BMI) using the link below –
A Family Disease: The Contagion of Habit
We need to stop viewing obesity as an individual failing. Obesity today is a family disease. In our clinics / OPDs, we rarely see one obese individual in a vacuum; we see entire households struggling.
While genetics may “load the gun,” it is the shared home environment that pulls the trigger. When parents struggle with weight, their children are often already on a trajectory toward metabolic dysfunction before they even reach puberty. We are raising the first generation of children who may have a shorter life expectancy than their parents.
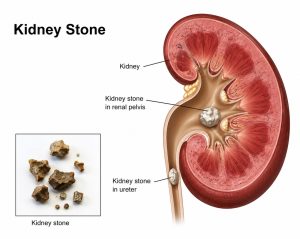
The Danger in the Middle: Central Obesity
While the total weight matters, where you carry it is even more critical. Central obesity, that stubborn belly fat, is not just storage. It is a metabolically active “organ” that pumps out toxins and inflammatory cytokines. This visceral fat wraps around your liver, heart, and kidneys, directly causing Type 2 Diabetes and metabolic syndrome.
Do you have Central Obesity?
To determine if you have central obesity objectively, you cannot rely solely on the bathroom scale. Total weight doesn’t tell us where the fat is stored, and as we’ve discussed visceral fat (the fat around our organs) is the primary driver of metabolic disease.
Here are the three most objective, clinically recognized ways to measure it at home or in a clinic:
1. Waist Circumference (The Gold Standard for Self-Assessment)
This is the simplest and most effective objective measure. It directly correlates with visceral fat levels and cardiovascular risk.
- How to measure: Stand up and place a tape measure around your middle, just above your hipbones. Make sure the tape is horizontal and snug, but not compressing the skin. Exhale normally and take the reading.
- The “Danger” Thresholds:
- Men: Over 90 cm (35 inches) for South East Asians; over 102 cm (40 inches) for Caucasians.
- Women: Over 80 cm (31 inches) for South East Asians; over 88 cm (35 inches) for Caucasians.
2. Waist-to-Hip Ratio (WHR)
This identifies your “shape” – specifically whether you are “apple-shaped” (storing fat centrally) or “pear-shaped” (storing fat in the hips/thighs).
- How to calculate: Divide your waist measurement by your hip measurement (taken at the widest part of your buttocks).
- Objective Risk: * Men: A ratio of 0.90 or higher indicates central obesity.
- Women: A ratio of 0.85 or higher indicates central obesity.
3. Waist-to-Height Ratio (WtHR)
Many experts believe this is the most accurate predictor of obesity-related cardiovascular risk because it adjusts for a person’s frame.
- The Simple Rule: Your waist circumference should be less than half your height.
- The Math: Waist/Height<0.5.
- Interpretation: If your waist is more than half your height, you are at a significantly increased risk for Type 2 Diabetes and heart disease.
Why “Normal BMI” Can Be Deceiving
It is possible to have a “normal” BMI but still have central obesity. This is often referred to as TOFI (Thin on the Outside, Fat on the Inside). In South East Asian populations, this is incredibly common. You may look lean in your arms and legs, but if your waist circumference exceeds the limits above, your internal organs are likely encased in inflammatory visceral fat.
A Health Toll Worse Than Drinking or Smoking:
We have spent decades rightfully vilifying smoking and excessive alcohol consumption. However, clinical data now suggests that the mortality risk of morbid obesity is reaching parity with long-term heavy smoking. If you wouldn’t hand your child a cigarette, why are we complacent about the skyrocketing rates of childhood obesity?
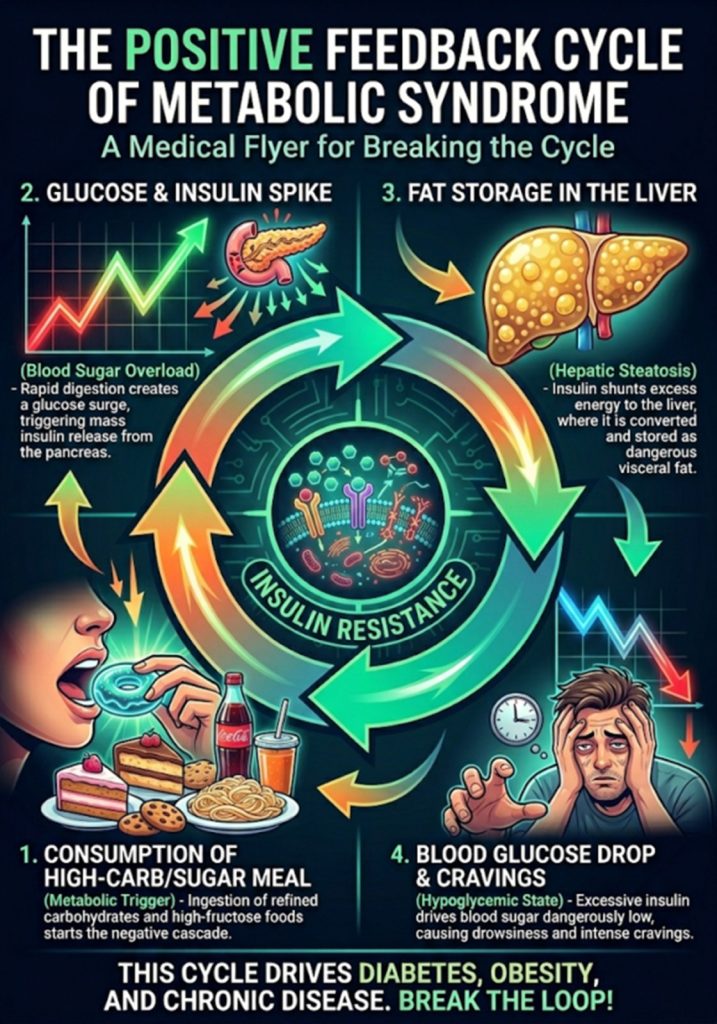
The Root of the Rot: Sugar, Carbohydrates, and the “SNACK” Trap:
The primary drivers of this crisis aren’t just lack of exercise; they are the substances we’ve normalized as “food.” Sugar and refined carbohydrates are at the dead center of this disease. When we consume high-glycemic carbohydrates, our bodies are flooded with insulin. Insulin is a fat-storage hormone. By constantly spiking it, we lock our bodies into a state where burning stored fat becomes biologically impossible.
This is compounded by the modern snacking culture. We have abandoned the concept of “three square meals” for a continuous “grazing” model. Every time you reach for a “healthy” granola bar or a bag of chips, you are re-triggering that insulin spike. This constant snacking means our metabolism never gets a break, leading directly to Central Obesity.
The Cardiovascular and Cancer Connection:
The risk to our heart increases exponentially with every point our BMI rises. But perhaps more terrifying is the Cancer Link. Obesity is now a leading cause of preventable cancer.
- For Women: The risk is especially harrowing. Adipose tissue (fat) produces estrogen. Excessive fat leads to a hormonal “overload,” significantly increasing the risk of breast, endometrial, and ovarian cancers.
- Reproductive Health: We are seeing an explosion of PCOS (Polycystic Ovary Syndrome) and infertility. For many couples, the barrier to parenthood isn’t a lack of technology; it’s the metabolic chaos caused by excess weight.
The Financial “Fat Tax”: Insurance Premiums:
The healthcare community is sounding the alarm, and the insurance industry is listening. Just as smokers pay higher premiums for their habit, we are approaching a reality where obesity-related health surcharges will become the norm.
Actuaries are looking at the data: the increased risk of strokes, heart attacks, and chronic dialysis. If the health risks don’t startle you, the financial impact of being “uninsurable” or priced out of the market should.
The Time to Move is “NOW”:
This is not a blog post about “body positivity”, this is a medical intervention. We are in a state of population-wide emergency. Every day you remain in a state of obesity, you are essentially “smoking” your internal organs.
The risks of mortality, the loss of quality of life, and the burden on our healthcare system are unsustainable. We need to wake up before the “silent pandemic” becomes a permanent reality for our children.
To truly “startle” yourself into action, you need more than just a body fat percentage. You need to see your future—specifically, your risk of a heart attack or stroke in the next 10 years. As a physician, I suggest you use these objective clinical tools to know that while you may feel “fine” today, your internal metabolic clock is ticking.
Know Your 10-year Individual Risk:
If you are serious about moving toward a healthier state, I recommend you have the following numbers ready before clicking these links:
- Systolic Blood Pressure (The top number)
- Total Cholesterol & HDL (From your last blood report)
- Your Waist Circumference (Measured at the navel)
Why these calculators are your best “Reality Check”
These tools take the “opinion” out of health. You can’t argue with an algorithm that says you have a 1 in 5 chance of a stroke before your children graduate.
1. The ASCVD Risk Estimator (The Global Standard)
The Atherosclerotic Cardiovascular Disease (ASCVD) risk score is the gold standard used by the American College of Cardiology. It predicts your 10-year risk of a “hard” cardiac event (heart attack or death).
- Best for: Adults aged 40–79.
- What it measures: It combines your cholesterol, blood pressure, and diabetic status.
- The Link: ASCVD Risk Estimator Plus
- The “Startle” Factor: If your score is above 7.5%, you are considered at “elevated risk.” If it’s above 20%, you are in a high-risk medical emergency zone.
2. QRISK®3 (The Most Comprehensive)
The QRISK3 is widely used in the UK and is often considered more “personal” because it includes factors the ASCVD misses – like your ethnicity (crucial for South East Asians), your BMI, and even conditions like migraines or severe mental illness.
- Best for: Getting a “Heart Age.” It tells you if your heart is biologically older than you are.
- The Link: QRISK3 Calculator
- The “Startle” Factor: It provides a “Healthy Heart Age.” Seeing that your 45-year-old body has the heart of a 65-year-old is often the wake-up call patient’s need.
3. WHO Cardiovascular Risk Charts (Specific for South East Asia)
Because South East Asians have a higher risk at lower BMI levels, the World Health Organization (WHO) developed region-specific charts. These are “non-laboratory” versions, meaning you don’t even need a blood test—just your age, smoking status, systolic blood pressure, and BMI.
- The Link: WHO South East Asia Risk Charts (PDF)
- How to use it: Find your age group and follow the color-coded grid.
- The “Startle” Factor: Dark Red cells indicate a >30% chance of a major cardiac event in the next 10 years.
**Patients who “see their risk” in black and white are 300% more likely to stick to a weight-loss protocol than those who are just told they “should lose weight.”
start today: do it for your health: do it for your families security
Dr. Somnath Chatterjee MD, FRCA, EDIC, FFICM
Medical Director
Prakriya Hospitals, Bengaluru