A Historic Milestone in the Fight against Anti-microbial resistance: Saluting Kerala’s Visionary Initiative
As a doctor I have spent decades in the wards and ICUs. I have watched with growing alarm and helplessness as our most potent weapons against infection – antibiotics – are failing us and our patients. Every day, I see patients in our ICUs and wards battling resistant superbugs. Infections that once were easily cured are now life-threatening. The rise of Antimicrobial Resistance (AMR) is not a distant threat; it is a silent pandemic happening in our hospitals and communities.
In the face of this gathering storm, true leadership and actionable vision are rare. This is why I am writing today with immense pride, profound hope, and heartiest congratulations for the Government of Kerala, and specifically the Hon’ble Health Minister, Mrs. Veena George (Journalist turned Politician). Kerala has officially become the first sub-national entity in the world to operationalize a standardized, tiered accreditation system for Antibiotic Smart Hospitals (ASH). This is a historic achievement that moves beyond policy, it is a life-saving intervention that sets a global benchmark.
What is Antimicrobial Resistance (AMR)?
AMR occurs when bacteria (germs) evolve to withstand the drugs used to kill them. The bacteria become resistant, not the person. If you get a resistant infection, common drugs won’t cure you, leading to longer hospital stays, much higher costs, and a higher risk of death.
The Gravity of the Silent Pandemic
To understand why Kerala’s success is so monumental, we must look at the grim reality of AMRIt is often called the “Silent Pandemic” because its victims aren’t always in the headlines, but the numbers are staggering.
According to the latest global data, bacterial AMR is associated with an estimated 4.95 million human deaths annually. Without drastic action, we are rapidly heading toward a “post-antibiotic era” where routine surgeries, C-sections, and even minor scratches could once again become fatal.
A Decade of Global Awakening: From 2015 to the 2030 Vision
The world began to wake up to this crisis in the mid-2010s. In May 2015, the World Health Assembly adopted the Global Action Plan on Antimicrobial Resistance, urging nations to develop their own strategic frameworks. This was the first time the global community recognized AMR as a threat to national security and economic stability.
Fast forward to the early 2020s, and the urgency has only intensified. During the 79th UN General Assembly in September 2024, world leaders signed a historic political declaration. The target is clear and ambitious: to reduce the 4.95 million annual deaths by 10% by the year 2030. To achieve this, the WHO has outlined concrete steps:
- Ensuring 70% of global human antibiotic use comes from the “Access” group (low-resistance risk).
- Ensuring 100% of countries have basic water, sanitation, and hygiene (WASH) services in healthcare facilities.
- Establishing sustainable financing to develop new medicines and rapid diagnostic tools.
A World First: Kerala Sets the Gold Standard
Kerala, a state known for its emphasis on public health, has etched its name in medical history by becoming the first state in the world to operationalize a comprehensive, tiered accreditation system – Antibiotic Smart Hospitals (ASH) as part of the initiative to become a 100% antimicrobial literate state and antibiotic literate Panchayats. This is not merely a policy statement; it is a groundbreaking operational framework that transforms how we use antibiotics from the primary health center up to the super-specialty Hospitals.
Health Minister Mrs. Veena George’s leadership in championing the Kerala Anti-Microbial Resistance Strategic Action Plan (KARSAP) and the Antibiotic Smart State initiative is an act of globally significant vision. By standardizing practices, demanding accountability, and creating a scalable model, Kerala is showing the rest of the world how to move from rhetoric to results in the fight against AMR. As on the date of writing this blog, 83 hospitals have been declared antibiotic smart and 5 Panchayats have been declared as antibiotic literate.
To Health Minister and her team at the Kerala Health Department – I laud your courage and vision. I also thank the state of Kerala for giving doctors and healthcare administrators like me a beacon of hope.
What is an ‘Antibiotic Smart Hospital’?
While many hospitals have existing antibiotic stewardship programs, the Kerala initiative is unique because it defines, standardizes, and certifies the practice through a rigorous checklist (ranging from 10 points for Primary Care to 15 points for Tertiary Care).
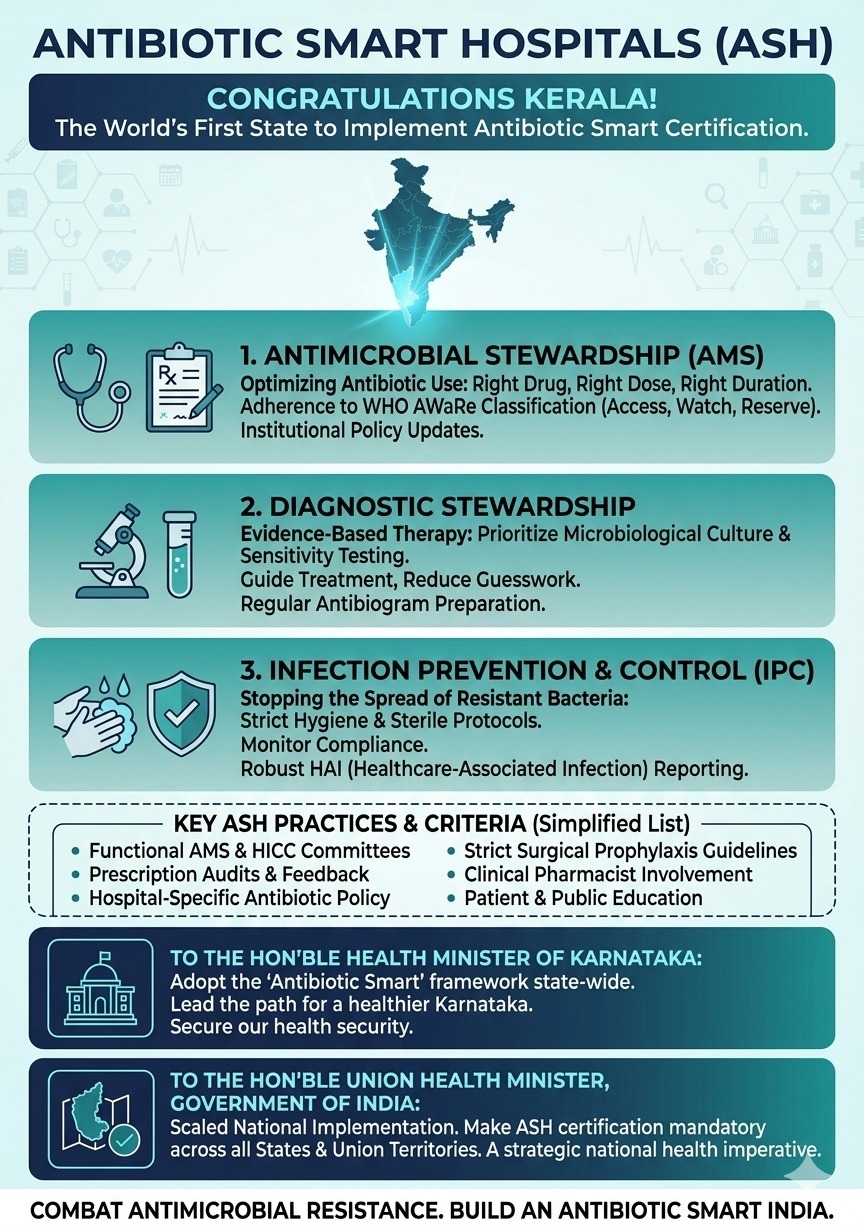
An ASH is an institution that rigorously commits to a “Theragnostic Model,” meaning its approach to therapy is tightly bound to diagnostic precision. This system moves beyond individual clinician choice and implements institutional rules. It rests on three essential pillars:
- Antimicrobial Stewardship (AMS): Ensuring the right patient gets the right antibiotic, at the right dose, by the right route, and for the right duration.
- Diagnostic Stewardship: The optimized use of microbiological culture and sensitivity testing to guide therapy, rather than relying solely on empiric (guesswork) broad-spectrum antibiotics.
- Infection Prevention & Control (IPC): Ensuring the hospital environment, hand hygiene standards, and sterile procedures prevent resistant bugs from spreading in the first place.
This structured approach is what makes the Kerala model “Smart”, evidence-based, data-driven, and institutionalized.
The 15-Point Checklist for Tertiary Care Hospitals
To be certified as an Antibiotic Smart Hospital, institutions must meet the following criteria:
- HICC & AMS Committees: Must have a functional Hospital Infection Control Committee (HICC) and an Antimicrobial Stewardship (AMS) Committee meeting at least quarterly.
- Institutional Antibiotic Policy: A written, evidence-based hospital-specific antibiotic policy updated every 6 – 12months.
- AWaRe (Access, Watch and Reserve) Classification Adherence: At least 90% of antibiotic prescriptions in general wards must be from the “Access” category (WHO classification).
- AWaRe Display: Posters explaining the “Access, Watch, and Reserve” groups must be displayed in all prescribing areas.
- Antibiogram Preparation: The Microbiology department must release a hospital-wide antibiogram every 6 to 12 months.
- Prescription Audits: Regular audits of antibiotic prescriptions must be conducted by the AMS team, with feedback provided to clinicians.
- Diagnostic Stewardship: Compulsory culture and sensitivity testing before starting “Reserve” category antibiotics.
- Surgical Prophylaxis Protocol: Standard Operating Procedures (SOPs) for pre-operative antibiotics must be strictly followed (e.g., giving the dose within 60 minutes of incision).
- Clinical Pharmacist Involvement: A dedicated clinical pharmacist must be part of the AMS team to monitor dosage and drug interactions.
- Documentation of Duration: The “Stop Date” or “Review Date” for every antibiotic must be clearly mentioned in the patient’s chart.
- Justification for ‘Reserve’ Drugs: Use of Reserve antibiotics (like Colistin or Linezolid) requires a “Reserve Drug Form” or justification by a senior consultant.
- Infection Prevention (IPC): Hand hygiene compliance must be monitored and documented regularly (above 70% target).
- HAI Reporting: Mandatory reporting of Healthcare-Associated Infections (like VAP or CLABSI) to the state AMR cell.
- Staff Training: 100% of clinical and nursing staff must undergo an annual AMR awareness training module.
- Patient Education (IEC): Malayalam/English posters for patients explaining why antibiotics aren’t needed for common colds or viral fevers.
An Urgent Appeal to the Public: Our Shared Responsibility
While hospitals must improve their systems, the battle against AMR can only be half-won without the support of the public. The demand for antibiotics from patients is a massive driver of resistance. I appeal to you, the general public: we need your help.
The Warning: The Consequences of Undisciplined Use
If we continue to use antibiotics indiscreetly, we face a “post-antibiotic era”:
- Simple operations like C-sections or joint replacements could become fatal due to untreatable post-surgical infections.
- Routine infections like urinary tract infections (UTIs) could lead to incurable sepsis.
- Higher, more toxic “Reserve” antibiotics (our last line of defense) will fail, leaving us helpless.
Instructions for Careful Use of Antibiotics:
- Never Use Antibiotics for Viruses: Antibiotics only kill bacteria. They are useless against viruses that cause the common cold, the flu, and most sore throats. Asking your doctor for an antibiotic for a cold is asking for something that won’t help you and will speed up resistance.
- Never Self-Medicate: Never buy antibiotics over-the-counter without a prescription. Never use “leftover” antibiotics from a previous illness.
- Complete Your Course: If your doctor prescribes antibiotics, take them exactly as directed, and finish the entire course, even if you feel better. Stopping early leaves the toughest bacteria alive to multiply and become resistant.
- Do Not Share: Never give your antibiotics to someone else, and never take theirs. Different infections need different treatments.
To my Colleagues in White Coats:
We must move away from “prescribing by habit.” We must embrace the antibiogram, respect the “Access” category, and have the courage to tell a patient when an antibiotic is not needed.
A Call to Action for Karnataka and the Nation
Kerala has provided the roadmap; we must now choose to travel it.
To the Hon’ble Health Minister of Karnataka:
Karnataka is a recognized global hub for medical tourism and houses some of India’s premier healthcare institutions. However, the shadow of AMR looms just as large here. We have the capability, the infrastructure, and the medical expertise to lead.
We appeal to you, Hon’ble Minister, to follow Kerala’s lead. Let us not wait. Let us adopt a modified version of this state-wide framework. By prioritizing the ‘Antibiotic Smart’ model in Karnataka, we can protect the quality of care we offer and ensure the sustainability of our health systems. We must establish state-wide benchmarks that recognize hospitals leading this charge.
To NABH (National Accreditation Board for Hospitals & Healthcare Providers):
NABH has revolutionized the quality and safety standards in Indian hospitals. You are uniquely positioned to turn this initiative from a state-specific best practice into a national standard. We urgently appeal to NABH to integrate the core criteria of the ‘Antibiotic Smart Hospital’ into your existing accreditation standards. AMR management must become a non-negotiable component of safety accreditation.
To the Hon’ble Union Health Minister, Government of India:
We look to the Center for decisive, national leadership. AMR is not a state issue; it is a national security crisis. We cannot afford 28 different states to have 28 different approaches.
We appeal to you, Hon’ble Minister, to champion this cause. Let Kerala’s historic framework be the template. We urge you to work towards making the ‘Antibiotic Smart’ accreditation mandatory for all tertiary hospitals and large private hospitals across all States and Union Territories of India. A phased, mandatory national rollout is necessary to avoid a healthcare apocalypse. Kerala has lit the flame; it is now the Union Government’s duty to carry that torch to every corner of India.
Kerala has lit the torch. It is now up to the rest of India to carry it forward. Let us build an Antibiotic Smart India before the miracle of antibiotics disappears forever. Let us together ensure that the miracle of antibiotics continues to save lives for generations to come.
Dr. Somnath Chatterjee MD (Anaes), FRCA, CCST, EDIC, FFICM
Medical Director, Prakriya Hospitals
Bengaluru