END OF LIFE CARE (EOLC) IN INDIA
Dr. Somnath Chatterjee, Medical Director, Prakriya Hospitals, Bengaluru
For the last several decades, families of patients have sat at the bedsides of their loved ones where medicine had reached its limit. For them, the hardest part wasn’t the physical pain of the patient; it was the “legal and moral limbo” that they were trapped in. They were forced to watch their loved ones exist in a shadow-land of machines, unable to recover, yet legally tethered to a life that had lost all its essence.
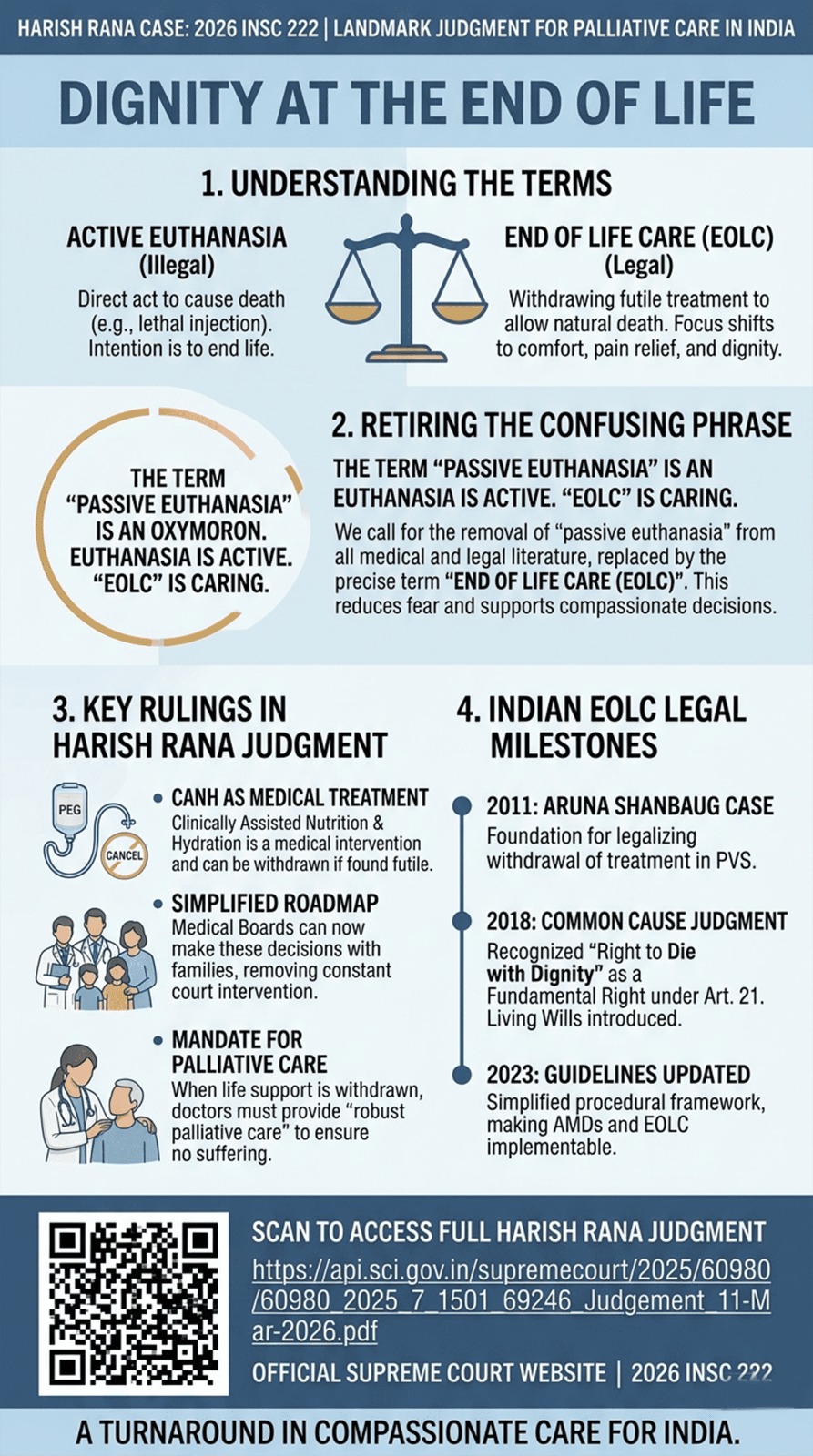
The recent Supreme Court judgment in the Harish Rana case (2026) is another turning point the medical (especially the Critical Care and Palliative Care) fraternities have been waiting for. But to truly understand it, we must first fix the way we talk about life, death, and the care in between.
Why the Harish Rana Case Changes Things Significantly
Mr. Harish Rana, a 32 year old gentleman, lay in a “persistent vegetative state” for over 13 years following a tragic accident. His brain had ceased to function, but his body was kept “alive” by a feeding tube. His family’s struggle eventually reached the Supreme Court. Here is why this judgment is a landmark:
- Feeding Tubes are “Medical Treatment”: The Court clarified that Clinically Assisted Nutrition and Hydration (CANH) – like feeding tube – is a medical intervention, not just “food and water.” If a treatment is futile, a doctor has a right (and a duty) to suggest stopping it.
- A Roadmap, Not a Roadblock: In the past, the process was complex and required the Primary and Secondary Medical Boards to opine and inform the Chief Judicial Magistrate. The Harish Rana judgment simplifies this, empowering Medical Boards to make these decisions with families.
- The Mandate for Palliative Care: The judgment explicitly states that when life-sustaining treatment is stopped, the doctor’s duty shifts to providing “robust palliative care” – ensuring the patient feels no pain or distress.
How the Harish Rana Judgment Improve on Previous Judgments
| Feature | 2018 Judgment | 2023 Amendment | Harish Rana (2026) |
| Magistrate Role | Mandatory visit & approval. | Informed after the decision. | Remains informed; focus shifts to clinical best interest. |
| Feeding Tubes | Ambiguous status. | Generally avoided. | Clearly defined as Medical Treatment. |
| Wait Period | Mandatory 30 days. | Mandatory 30 days. | Can be waived in cases of obvious futility. |
| Board Readiness | Ad-hoc / Difficult to form. | Simplified composition. | Standing panels mandated at District level. |
| Post-Withdrawal | No specific mandate. | General guidance. | Mandatory “Robust Palliative Care” plan. |
The Need for Considerate Implementation
While the law has cleared a path, we must walk it with extreme care. Transitioning a patient to End-of-Life Care is not like flipping a switch. It requires:
- Deep Communication: We must sit with families, often for hours, to ensure they understand that stopping a machine is not “giving up” or “causing death” – it is an act of profound love and mercy.
- Symptom Management: As we withdraw machines, our focus intensifies on comfort. We use medication to ensure there is no gasping for breath, no pain, and no agitation.
- The “Best Interest” Standard: Every decision must be centered on the patient. Would Harish have wanted to be remembered this way? Does this treatment offer him any benefit, or only the burden of continued existence?
Clearing the Confusion: What is “Euthanasia”?
In the medical and legal world, we have traditionally split euthanasia into two categories. It is vital to understand the difference:
- Active Euthanasia: This is a direct, intentional act to end a patient’s life, such as administering a lethal injection. In India, this remains illegal.
- “Passive Euthanasia”: This refers to the withdrawing or withholding of life-sustaining treatments (like ventilators or feeding tubes) when they are no longer helping the patient and are only prolonging the process of dying. This is legal under specific guidelines.
The Problem with the Words We Use
As a Critical Care physician, I believe it is time we stop using the phrase “passive euthanasia” altogether. To most people, the word “euthanasia” implies an active choice to end a life. Adding the word “passive” in front of it doesn’t make it sound any less frightening to a grieving daughter or a hesitant doctor. In fact, it’s a contradiction in terms. Euthanasia is, by definition, an active intervention.
The phrase “Passive Euthanasia” needs to be abandoned
In mature medical and legal systems – particularly in the UK, USA, Australia, and much of Western Europe – the phrase “passive euthanasia” has been largely abandoned in official discourse. It is now considered an archaic, inaccurate, and ethically confusing term.
Instead, these jurisdictions use precise, clinical language that reflects the reality of medical practice: the limitation of life-sustaining treatment or End-of-Life Care (EOLC).
The Shift in Terminology
The medical fraternity in these regions argues that “Euthanasia” is an active act with the intent to kill. Combining it with “Passive” creates a linguistic oxymoron that leads to the following misconceptions:
- The Intent: In EOLC, the intent is to relieve suffering and allow a natural death, whereas in Euthanasia, the intent is to end life.
- The Cause of Death: In EOLC, the cause of death is the underlying disease. In Euthanasia, the cause of death is the intervention (the drug).
Current Terms used Globally
| Country/Region | Former Term | Current Legal/Medical Terminology |
| United Kingdom | Passive Euthanasia | Withdrawing or Withholding Life-Sustaining Treatment (LST); Decisions to Forego Life-Sustaining Treatment. |
| United States | Passive Euthanasia | Allowing Natural Death (AND); Foregoing Life-Sustaining Treatment; End-of-Life Care. |
| Australia | Passive Euthanasia | Limitation of Medical Treatment; Voluntary Assisted Dying (VAD) is used strictly for active assistance, while withdrawal is simply “standard medical practice.” |
| Europe (EAPC) | Passive Euthanasia | End-of-Life Decisions; Palliative Care Strategy. |
We need to retire this phrase and replace it with what we actually practice: End-of-Life Care (EOLC). hen we stop a machine that is no longer working, we aren’t “killing” the patient; we are simply stepping out of the way and allowing nature to take its course. We are shifting our focus from prolonging the dying process to supporting the living person until their last breath. Using the term EOLC removes the “stigma of the act” and replaces it with the “promise of care.”
A New Vocabulary for a New Era
The “Passive Euthanasia” label has caused enough fear. It makes doctors afraid of being called “killers” and makes families feel like they are betraying their loved ones.
By embracing the term End-of-Life Care, we acknowledge that medicine has a natural limit. We acknowledge that “dignity” is not just a word in a court document, but a reality we create at the bedside.
The Harish Rana case has finally bridged the gap between law and mercy. It allows us to stop being mechanics of the body and return to being healers of the person. Let us use this moment to start having honest, brave conversations about how we wish to be cared for at the end of our journey.
*** Note to Readers: Palliative care and EOLC are about specialized medical care for people living with a serious illness. This care is focused on providing relief from the symptoms and stress of the illness. The goal is to improve quality of life for both the patient and the family.