A Choice of Necessity, Not Neglect
Doctors are Victims of a Broken System
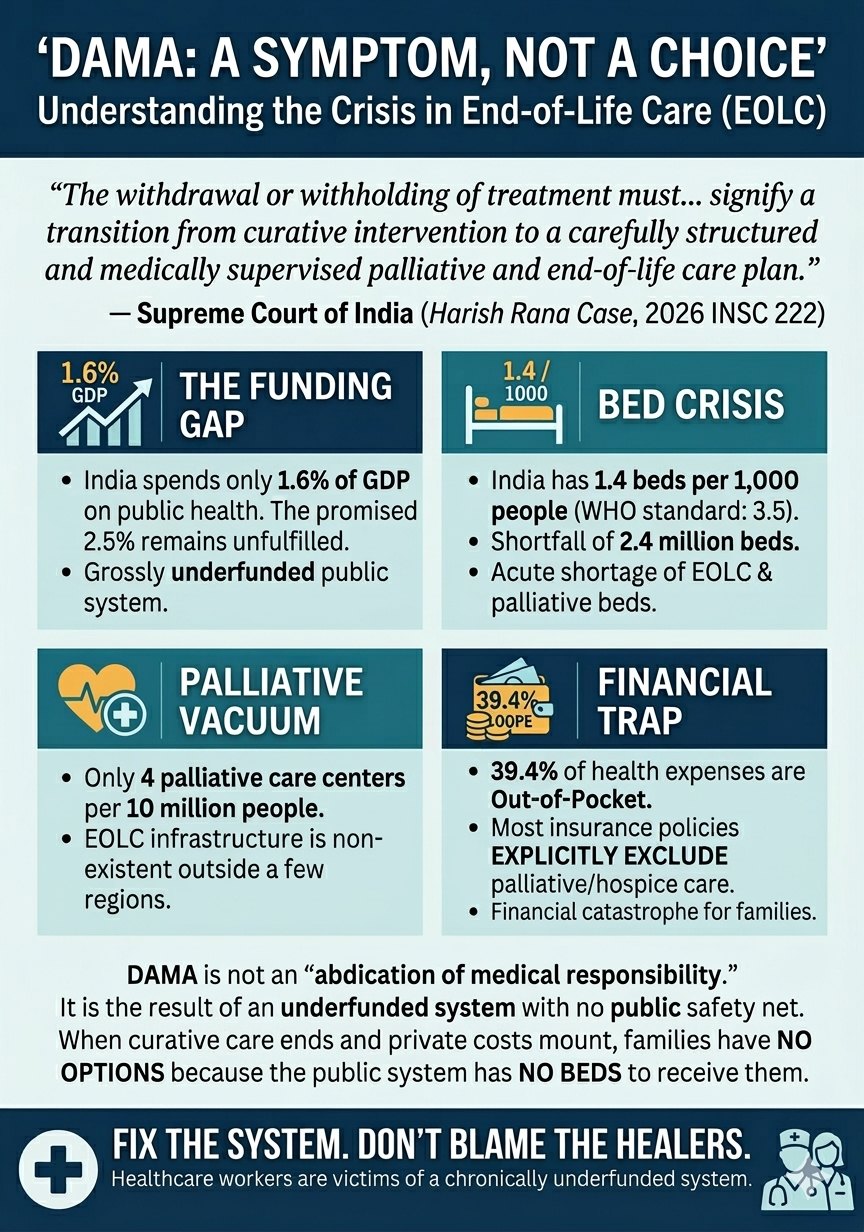
The recent Supreme Court judgment in the Harish Rana case (2026 INSC 222) has sent ripples through the Indian healthcare community. In a landmark ruling, the bench of Justices J.B. Pardiwala and K.V. Viswanathan expressed deep concern over the practice of “Discharge Against Medical Advice” (DAMA), warning that it often amounts to an “abdication of medical responsibility.”
The court stated verbatim:
“We strongly disapprove of the routine practice of ‘discharge against medical advice’… which is misused in situations where medical treatment stands discontinued. Resorting to such a course of action… risks amounting to an abdication of medical responsibility and undermines the very rationale of treatment limitation.”
As a sincere doctor with a very strong sense of responsibility, I have no hesitation in expressing that I am deeply hurt by the sentiments expressed in the paragraph above. I have highlighted the words or phrases that hurt me immensely. DAMA is definitely not routine. The decision to send a patient DAMA is only taken if there is no other option. The word “misuse” is absolutely opposite to the sense of helplessness I feel when I have no other option available to offer. The phrase “risks amounting” conveys a veiled legal threat. Such generalizations do immense disservice to the countless doctors who give their heart and soul to the science and craft of medicine.
I want to speak directly to the public, the media, and our legal system. We are not abdicating our responsibility. We are struggling to survive within a system that is failing both the patient and the provider.
Below are some examples of what we have done in the last three months to prove that we take our responsibility seriously –
- ~ 80 year old lady. Severe viral pneumonia. Following 10 – 12 days of aggressive ICU care despite repeated poor prognostication of the family finally agreed to opt for the palliative care option. The patient had expressed a wish to be cremated in her village in North Karnataka. In this section of North Karnataka, one is not allowed to be cremated in the village if they do not die in the village (as informed by family). We transported her 200 Km in an ambulance on 100% Oxygen on a ventilator and extubated her at home following palliative sedation administration so that her final wish could be fulfilled.
- A young lady in advance pregnancy with severe heart disease due to scarring of her heart valve collapsed in a hospital 100+ km away from Bangalore. She was rushed to Bangalore in an ambulance. She was very sick and our hospital was the 7th hospital she approached for help. We took her to the ICU. Delivered the babies and treated her for couple of days. The family requested us to discharge her against medical advice because they could no longer afford treatment. We refused to let her die in the back of an ambulance. We knocked on every door till we could get through the Medical Superintendant of Centre of Excellence of a public hospital who proactively helped her be safely transferred to the ICU in her hospital. Thank you Madam.
- A young man aged ~ 25 years suffered a cervical spine injury leaving him quadriplegic (unable to breathe or move his upper and lower limbs). He was stabilized in our ICU and after 7 – 10 days, the parents expressed their inability to pay for his further care and wanted to take him to Chennai to a Government Hospital. Our team ensured that he was transferred safely nearly 300km to Chennai so that his treatment could continue in the Government hospital.
The above are just few of the examples of the proactive compassionate and responsive care we as a team delivered to our patients in their hour of need.
The Systemic Trap: Why DAMA Really Happens
When a patient reaches the end of their life in a private or corporate hospital, the transition from “curative care” to “palliative care” is not just a medical decision – it is a financial and legal crisis.
DAMA happens because our healthcare system is a victim of decades of underfunding. Consider these cold, hard facts:
- The Underfunding Crisis: For years, the government promised to increase public health spending from 1% to 2.5% of GDP. Today, we still hover around 1.6% to 1.9%. In contrast, developed nations spend 7–12%, and even our neighboring countries excluding Bangladesh and Pakistan (Nepal, Bhutan and Sri Lanka) spend 2 – 3% of their GDP. Should we not be asking – why this malaise?
- The Bed Deficit: India has roughly 1.4 hospital beds per 1,000 people. The WHO standard is 3.5 beds / 1000 people. In the public sector alone, that number drops to a staggering 0.79 beds. We are short by an estimated 2.4 million beds.
- The Palliative Care Vacuum: The Supreme Court suggests we should transition patients to a “structured palliative care plan.” But where are the beds? India has only 4 palliative care centers for every 10 million people. Outside of Kerala (which holds nearly 45% of India’s palliative infrastructure), the availability is almost zero.
- The Out-of-Pocket Burden: Despite schemes like Ayushman Bharat, 45 -50% of health expenditure in India is still Out-of-Pocket (OOPE). In private hospitals, this number is often 100% for the “missing middle.”
The “Moral Injury” of the Private Sector
The less fortunate section of the Indian population is unable to afford for curative treatment in the private hospitals, forget about paying for palliative care. Is it a fair ask from the private hospitals to provide palliative care for free?” The private healthcare sector provides nearly 50 – 55% of the care in this country. SME hospitals (less than 200 beds) operate on thin margins of profit (most often single digit) compared to large corporate hospitals, especially in Tier 2 and 3 cities. Unfortunately, a private hospital cannot provide end-of-life care without reimbursement.
Does insurance cover palliative care?
The answer, largely, is NO. Most Indian insurance policies explicitly exclude “palliative therapy” or “hospice care” if active hospitalization is not required. If the insurance industry is not forced to cover End-of-Life Care (EOLC), the burden falls entirely on the family. When a family’s savings are exhausted, and the public sector has no palliative bed to offer, DAMA is the only remaining door.
Decades of Legal Fear
For decades, EOLC in India has been in its infancy. The 2018 Common Cause judgment was procedurally complicated – requiring judicial magistrates and multiple boards – that it created a climate of fear. Doctors were terrified that withdrawing a ventilator, even for a terminal patient, would lead to a murder charge.
The Harish Rana case has finally brought much-needed clarity, but it does not fix the broken pipes of our infrastructure.
A Plea for Faith, Not Friction
The medical community operates in a defensive position. We face constant negative sentiment from the media and a lack of faith from the judiciary. We see our colleagues physically harmed, and even killed, for doing their duty. While laws exist to protect us, how many perpetrators are actually jailed?
The only time society showed us gratitude was during the peak of COVID-19. Today, we are back to being viewed with suspicion.
To the Public: The average doctor is honest. We are doing the best we can in a system we did not build and cannot fix. We are humans, not Gods. We cannot conjure a palliative bed where none exists, and we cannot force an exhausted family to pay for an ICU / hospital stay that has no hope of a cure.
To the Legal System and the Media: We invite you to see the reality behind the clinical forms. When the judiciary expresses disapproval of practices like DAMA, we feel the weight of that judgment deeply. However, constant criticism without systemic context only deepens the lack of trust. DAMA is the symptom of a systemic disease – an underfunded and over-leveraged health economy that we did not create, but are forced to manage. We are doctors, but we are also human. We ask for the same empathy the public expects from us – a mutual compassion that recognizes the impossible choices we face every day in an under-resourced system.
Dr. Somnath Chatterjee MD, FRCA, EDIC, FFICM
Medical Director
Prakriya Hospitals
Bengaluru