Are you worried about it?
If you answered “yes” to either of those questions, pull up a chair. As a pulmonologist who has spent years studying the science of sleep, I can tell you that snoring is far more than just a “nuisance” or a funny habit. It is often the smoke that indicates a fire – and that fire is happening inside your airway every single night.
What Exactly Is Snoring?
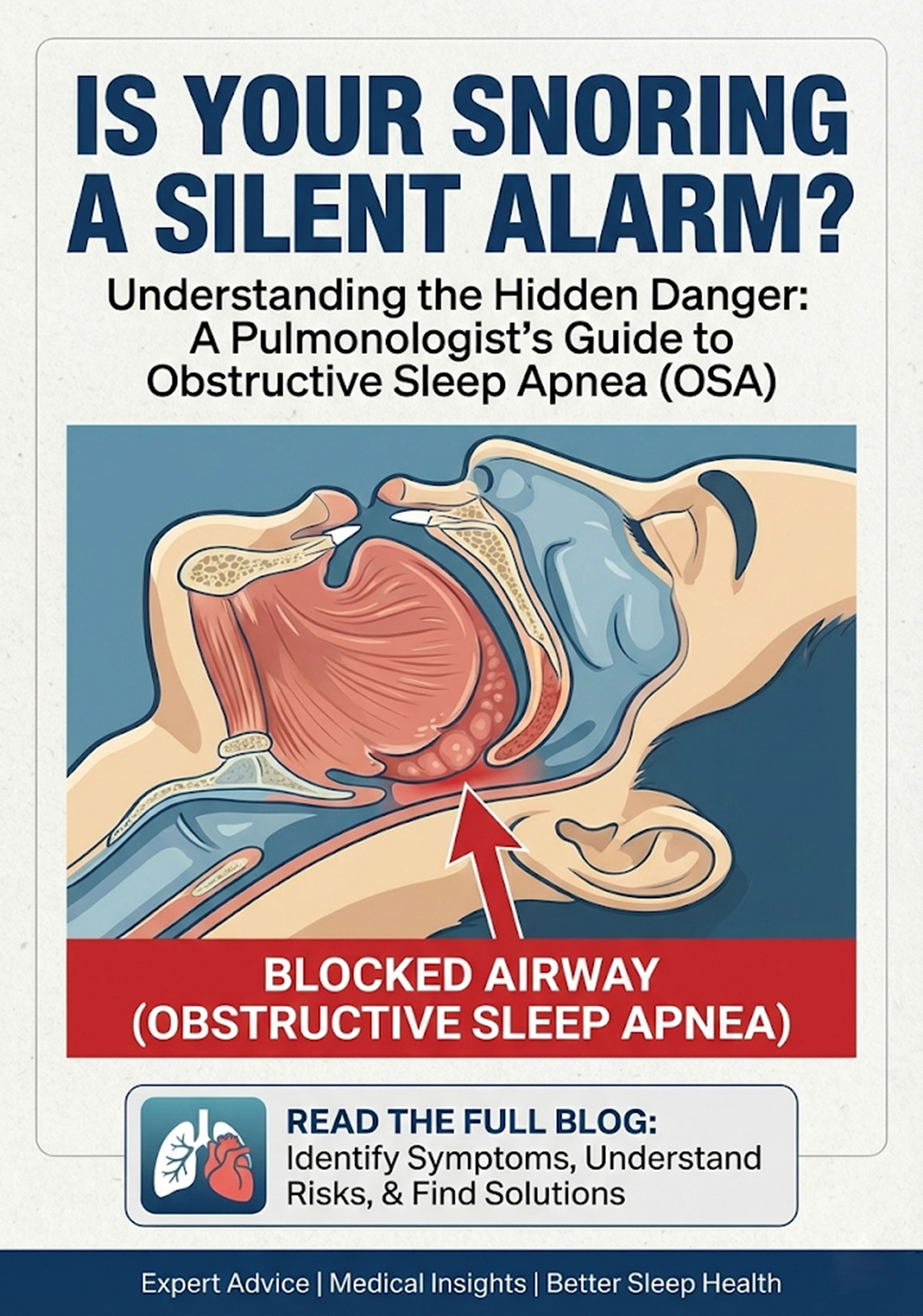
Think of your airway (breathing passages) as a flexible tube. When you sleep, the muscles in your throat, tongue, and soft palate relax. If they relax too much, or if there is extra tissue (usually fat) in the way, the airway narrows. As you breathe, the air has to force its way through this tight space, causing the soft tissues to vibrate.
That vibration is the sound we call snoring.
Is it always a problem? Not necessarily. “Simple snoring” happens occasionally (like after a glass of wine or when you have a cold) and doesn’t disrupt your oxygen levels. However, for many, snoring is the primary symptom of Obstructive Sleep Apnea (OSA).
When Snoring Becomes “Ominous”
Snoring becomes dangerous when it stops being a continuous sound and starts being a cycle of gasps, snorts, and silence. In OSA, the airway doesn’t just narrow; it collapses entirely. Your brain realizes you aren’t getting oxygen and sends a jolt of adrenaline to wake you up just enough to take a breath. This can happen 30, 60, or even 100 times per hour. You won’t remember these “micro-awakenings,” but your heart and lungs certainly do.
The Heavy Connection: Obesity and Snoring
There is a direct, scientific link between weight and snoring. When we carry excess weight, particularly around the neck, that fat puts physical pressure on the airway.
- The “Collapsing Tube”: Extra fat deposits (adipose tissue) in the walls of the throat make the “tube” narrower and more likely to collapse under the pressure of inhalation.
- Can weight loss help? Absolutely. Even a 10% reduction in body weight can significantly improve airway space and, in some cases, eliminate mild sleep apnea entirely.
What It Does to Your Body
Untreated OSA can lead to Uncontrolled diabetes, hypertension, serious Heart, Brain, and daily-life complications, some of which may be life-threatening.
- Oxygen Deprivation: Every time you stop breathing, your blood oxygen levels drop.
- The Adrenaline Spike: Your body enters a “fight or flight” mode to keep you alive, causing your blood pressure to spike.
- Pulmonary Hypertension: This is a condition where the blood pressure in the arteries of your lungs becomes dangerously high. Because the lungs aren’t getting enough oxygen, the blood vessels there constrict, forcing the right side of your heart to work much harder to pump blood.
- Heart Failure & Stroke: Over time, this “heavy lifting” weakens the heart muscle. Untreated severe snoring/OSA is a leading contributor to heart attacks, irregular heartbeats (atrial fibrillation), and early death.
- Cognitive impairment: Poor quality sleep leads to difficulty in concentration, memory problems, mood distrubances leading to work place and motor vehicle accidents
Treatment Options: From Masks to Scalpels
The good news? We have highly effective ways to fix this.
Medical Treatments:
- CPAP (Continuous Positive Airway Pressure): The “Gold Standard.” It’s a small machine that blows a gentle stream of air into a mask, acting like an “invisible splint” to keep your airway open.
- Oral Appliances: Custom-made mouthguards that pull your lower jaw forward to create more space in the back of the throat.
Surgical Treatments:
- UPPP (Uvulopalatopharyngoplasty): Removing excess tissue from the soft palate and uvula.
- Hypoglossal Nerve Stimulation: A small “pacemaker” for the tongue that keeps it from falling back into the throat.
My Advice to You
If you are waking up tired, falling asleep during the day, or if your partner tells you that you “stop breathing” or “gasp” at night, do not ignore it. This is not a sign of getting old; it is a treatable medical condition. By addressing your snoring, we aren’t just helping your partner get a better night’s sleep—we are protecting your heart, your brain, and your future.
When should you seek help? Right now. If you have high blood pressure, a thick neck circumference, or daytime fatigue, you need a Sleep Study (Polysomnography) to see what’s happening behind the scenes.
Demystifying the Sleep Study (Polysomnography)
It is a big step to move from “ignoring the noise” to “seeking a solution.” As your specialist, let me break down exactly what happens during a sleep study and what you should ask when you finally sit down in that specialist’s office.
Think of a sleep study as a “performance review” for your body while it’s off the clock. There are two main types:
- In-Lab Polysomnography (The Gold Standard): You spend the night in a private, hotel-like room at a sleep center. A technician applies small sensors to your head and body. It might look like a “mad scientist” experiment with all the wires, but it’s entirely painless.
- Home Sleep Apnea Test (HSAT): If your case seems straightforward, we might send you home with a simplified kit. It measures breathing and oxygen but doesn’t track brain waves.
What are we actually measuring?
We look at several data points to see how hard your body is working to stay alive while you sleep:
| Metric | What it tells us |
| EEG (Brain Waves) | What stage of sleep you are in (REM vs. Deep sleep). |
| Airflow & Effort | If you are trying to breathe but the “pipe” is blocked. |
| SpO2% (Oxygen Levels) | How low your oxygen drops during an apnea event. |
| ECG (Heart Rhythm) | If your heart is skipping beats due to the stress of gasping. |
| Leg Movements | If restless legs are contributing to your fatigue. |
Preparing for Your Appointment: Questions to Ask
Use these questions to ensure you get a comprehensive plan:
- “What is my AHI (Apnea-Hypopnea Index)?” (This is the number of times you stop breathing per hour. Under 5 is normal; over 30 is severe.)
- “How low did my oxygen saturation go?” (Anything below 90% is a concern; below 80% is high-risk territory.)
- “Based on my airway anatomy, am I a candidate for an oral appliance or just CPAP?”
- “Does my weight or my neck circumference play the biggest role here, or is it structural (like a deviated septum)?”
- “What are the long-term risks for my heart if I leave this untreated for another year?”
A Piece of “Doctor-to-Patient” Advice
Nothing is less appealing than being chronically exhausted, irritable, and at risk for a stroke. Most partners prefer the “white noise” of a machine to the terrifying silence of their loved one not breathing. This can be the difference between life and death.
Dr. Ravivarma A, MD, FIP
Consultant Pulmonologist
Prakriya Hospitals, Bengaluru
Dr. SomnathChatterjee MD, FRCA, EDIC FFICM
Medical Director
Prakriya Hospitals, Bengaluru