A 43 year old man, diabetic, who was diagnosed with sputum positive pulmonary tuberculosis and treated for the same, presented with hemoptysis of 6 months duration, 11 months after being diagnosed with pulmonary tuberculosis.
His symptoms persisted despite medical management.
Auscultation revealed bronchial breathsounds in right supraclavicular area with crepitations.
Total WBC count was 12320/cumm. Chest radiograph showed peribronchial opacities with increased bronchovascular markings in right upper zone with a doubtful cavity.
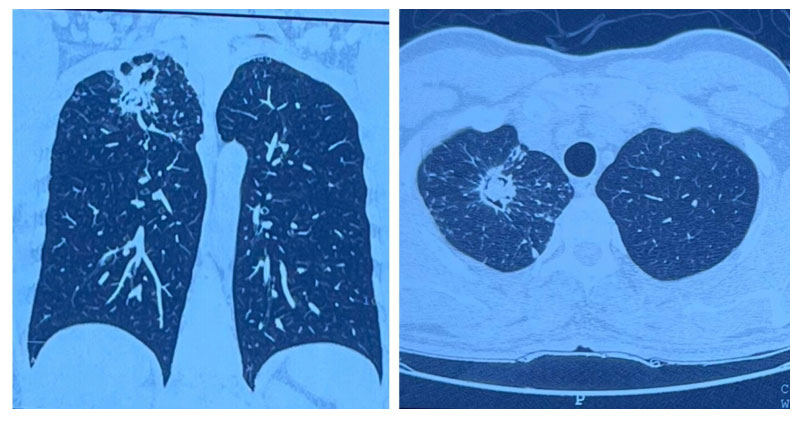
Computed tomography of the chest showed a thin walled cavitory lesion measuring 26 x 25x 17 mm with hyperdense content in the apical segment of right upperlobe with surrounding bronchiectatic and fibroatelectatic changes
Bronchoscopy revealed no abnormality.
In view of recurrent hemoptysis, patient was referred for surgical resection. Segmentectomy of right upper lobe apical segment was done and fungal structures were observed under a microscope, stained with lactophenol cotton blue.

Segment measuring 7 x 5 cm was obtained during the procedure. Cut section showed a cavity measuring 2 x 1.8 cm containing tangled mass of fungal fibres and necrotic material . Filamentous mold colonies which were fluffy, cottony, with radial growth and white-to-green powdery spores were seen. Findings were in concordance with Aspergillus flavus as it was greenish in colour in direct plate in Sabouraud Dextrose Agar.
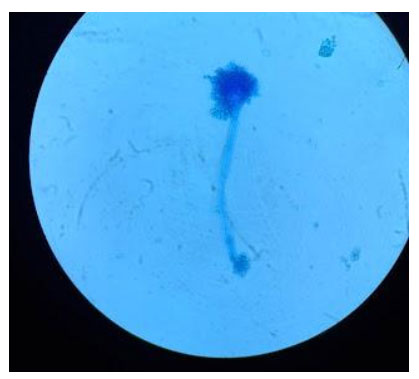
Septate hyphae with branching filaments were seen under microscope. Conidiophore with a vesicle and radiating conidia, typical of Aspergillus was observed
Patient was initiated on Voriconazole. He improved clinically and was discharged on oral antifungals for 2 weeks. Patient was followed up and had been asymptomatic and doing well.
Learning points:
● Chronic Pulmonary Aspergillosis (CPA) is a common complication of treated pulmonarytuberculosis with cavitation .
● The most common form of CPA is Chronic Cavitory Pulmonary Aspergillosis(CCPA).
● The most common species causing an aspergilloma is the Apergillus fumigatus.Aspergillomas form typically in pre-existing lung pathology, most commonly in oldhealed pulmonary tuberculosis cavities.
● The definitive treatment modality is still a topic of debate. Since the cavity and fungalball are avascular in nature, the medical treatment is not so effective, though antifungalscan be used to reduce the symptoms.
● The non-surgical treatment modalities like intra-cavity instillation of antifungal agentsand bronchoscopic removal of pulmonary aspergilloma have been reported only in smallretrospective studies and cannot be done in resource limited settings. Patients canundergo bronchial artery embolisation for hemoptysis as a temporary measure
● Surgical resection is the most effective treatment strategy for patients with aspergilloma,lobectomy being the most common procedure. Post operative complications includingprolonged air leak, bleeding, repeated pneumothorax, empyema and wound dehiscencecan be reduced by preoperative preparation, meticulous surgical technique and postoperative chest physiotherapy. Surgical resection is effective in preventing recurrence ofhemoptysis, and the long term outcome is good.
● Peri-/postoperative antifungal therapy is not routinely required, but suggested if there isrisk of surgical spillage of the aspergilloma, to prevent Aspergillus empyema andrecurrence of aspergilloma after surgical resection.
● Segmentectomy proves successful in a vast majority of aspergilloma cases, which has anextra edge of preserving a considerable part of the lung. Nevertheless, randomisedcontrolled trials are needed to establish the effectiveness of segmentectomy in operablecases and non-surgical treatment paradigm for inoperable cases
Dr. Divya Surendran
MBBS, MD Respiratory Medicine, EDARM
Consultant – Pulmonologist
https://www.prakriyahospitals.com/doctors/dr-divya-surendran.html